

2026 SS and Medicare Funding Status
Social Security and Medicare are very important programs. Social Security provides monthly income that grows with inflation for as long retirees live. Medicare provides health coverage during potentially vulnerable times. For those wondering if the programs will be around when they retire, the answer is yes, but benefits may be reduced and/or additional taxes required. Corrective action is long overdue. This post will provide a financial overview of these programs in a Q&A format.
Summary
I start with three graphs for those who want a quick summary. Following that are more details in an easy to consume Q&A format for more context and understanding of these very important programs. In summary, both Social Security (OASDI) and Medicare HI Trust funds are projected to run out one quarter sooner than last year’s estimate (combined OASDI in table below is 2034 and 83%). The Medicare portion covering doctor visits and drugs does NOT have a Trust fund so not projected to hit $0 but premiums will likely continue to increase.
Before I begin with the Q&A details, there are three important documents I encourage you to become familiar with:
- Social Security Statement - provides an estimate of your monthly benefit based on earnings history. Annual mailing of statements stopped in 2011 (may receive in mail if over age 60 and not registered online).
- A Summary of the 2026 Annual Report - provides an executive summary with more graphics and additional topics.
- Annual Trustee Report - shows the financial health of both programs and actuarial projections. The latest report was released June 9, 2026 with useful information and the main source for this blog, both the Summary and Trustees Report (273 pages) for those who want details!
Q1 - What programs are included in Social Security and Medicare and what is funding status?
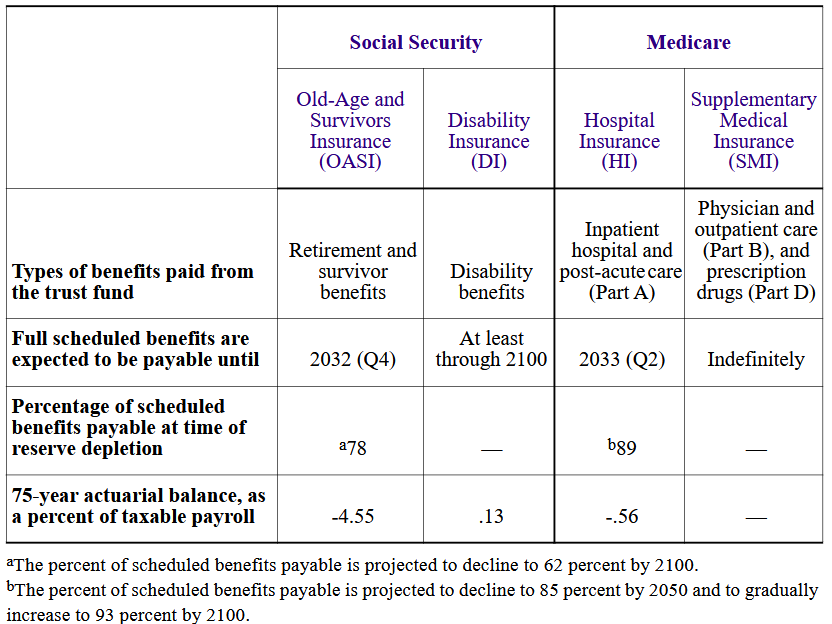
Social Security and Medicare are social insurance programs that provide benefits for individuals or family members for those workers who satisfy the number of years worked (and paid taxes) requirement. There are separate programs within both Social Security and Medicare, though it is common to refer to them as simply two programs. Each Social Security program has their own Trust Fund while only Medicare Part A (Hospital Insurance) has a Trust Fund. Medicare Part B and D are financed by a combination of premiums and large % from general tax revenue (more on that later!). Medicare Advantage Part C is financed by combination of premiums and working relationships with Government and private companies, but this program is NOT addressed in the Trustee Report.
Social Security (OASDI)
- Old-Age and Survivors Insurance (OASI) – pays retirees and survivors
- Benefits covered 100% to 2032, then 78%
- Past Few Years – ranged from 2033-2034 and covered 77-79%
- Disability Insurance (DI) – pays those unable to work due to disability
- Benefits covered 100% over next 75-year projection period (same as recent past)
- NOTE: combined OASDI 100% covered to 2034, then 83%
- Past Few Years – ranged from 2034-2035 and covered 80-83%
Medicare (Part A, B, D)
- Hospital Insurance (HI) – Medicare Part A (inpatient hospital care)
- Benefits covered 100% to 2033, then 89%
- Past Few Years – ranged from 2028-2036 and covered 89-90%
- Supplemental Medical Insurance (SMI) – Medicare Part B (physicians, outpatient care) and Medicare Part D (prescription drugs)
- Benefits covered 100% into future; just raise premiums and grab more tax revenue
- NONE of the FICA tax paid over the years covers this portion of Medicare!
- 22% of full cost covered my Medicare premiums you pay
- 75% of full cost covered by general revenue from taxpayers; 3% other
Medicare (Part C)
- Medicare Advantage – Medicare Part C combines Part A and B benefits, and some plans Part D
- NOT part of Trustee Report but mentioning here for completeness of programs
- Premiums paid by participants plus a relationship with Government + private companies
Q2 - Who pays for Social Security and Medicare?
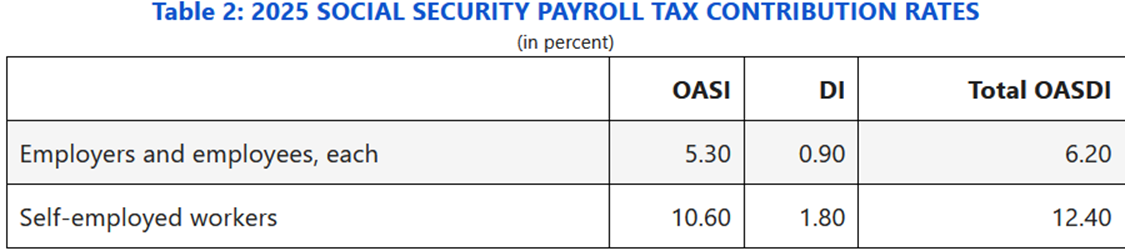
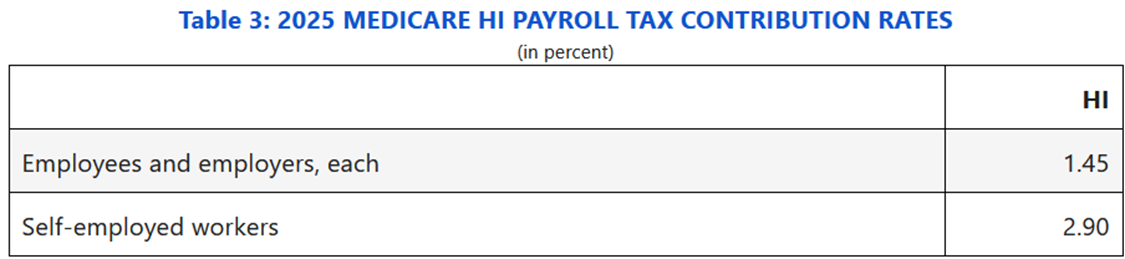
You do – either from payroll tax or general tax revenue, plus direct premiums if on Medicare. Current workers contribute a portion of their paycheck for the three programs in table below - sometimes called “payroll or FICA tax”. Your employer also pays the same tax; the self-employed pay the full 15.3%. The 6.20% OASDI tax applies to income up to $184,500 (for 2026) but the 1.45% Medicare tax is paid on all income. There is an additional 0.9% Medicare tax for the employee on earnings above $200,000 for individuals and $250,000 for joint filers that started in 2013 to help fund part of Affordable Care Act (not shown in table below). Also note the $200k and $250k is NOT indexed for inflation, catching more workers each year with wage inflation.
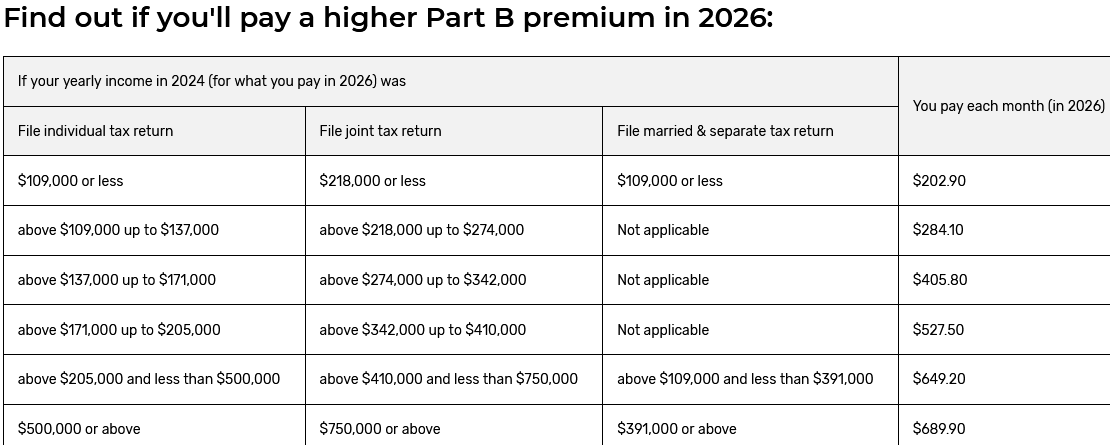
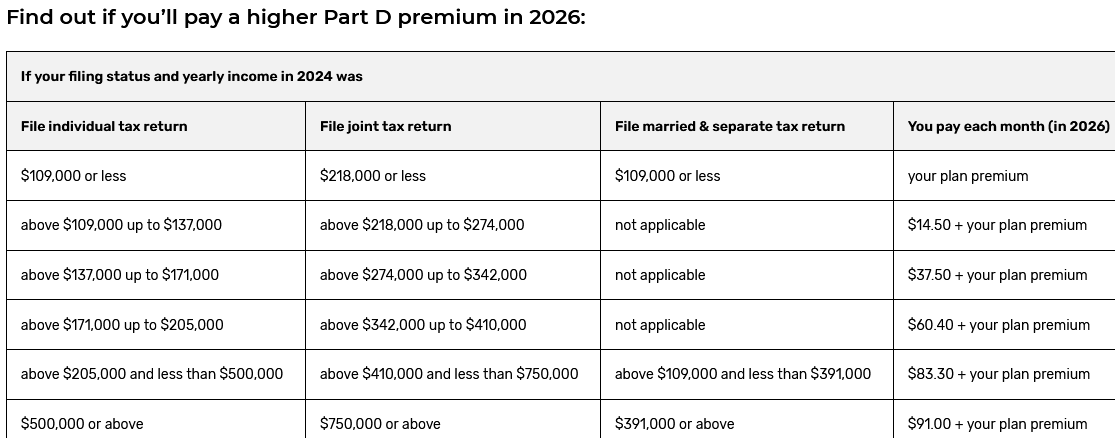
Medicare Part B and Part D is funded primarily from two sources – about 75% comes from general revenue of our generous taxpayers, 22% comes from monthly premiums by retirees and the remaining 3% from other sources. That’s right – the monthly Medicare premiums you pay only covers about 22% of the true cost! Medicare Part B monthly premium = $202.90/month in 2026; Part D base premium varies by plan depending on specific drug coverage you select. Additional tiered premiums for Part B and D are required for high income retirees (in 2026 – if Modified Adjusted Gross Income above $109,000 for individual filers; $218,000 for joint filers – more details later).
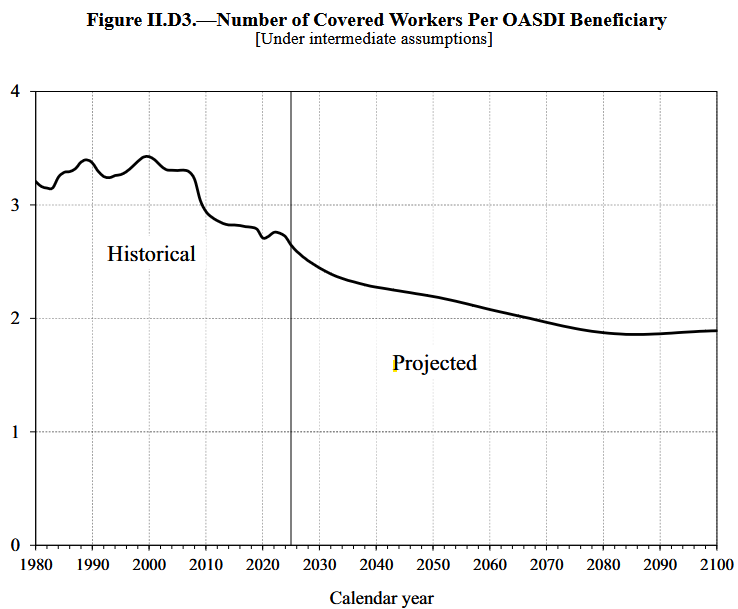
Q3 - Does each worker have their own account where the payroll taxes go until they retire?
No. Unlike your 401k account or savings account, Social Security and Medicare Part A use “pay-as-you-go funding”. This means payroll taxes collected by current workers are used to pay the bills for existing retirees. When existing workers retire, the next generation of workers will be paying their bills. Yes, the number of workers relative to the number of retirees changes over time and impacts the financing. The Social Security and Medicare actuaries project the expected financial impact on these changing demographics, but the tough part is convincing politicians and the public to make the tough choices now to assure long-term funding.
Q4 - What happen if there is extra payroll tax not needed to pay current benefits?
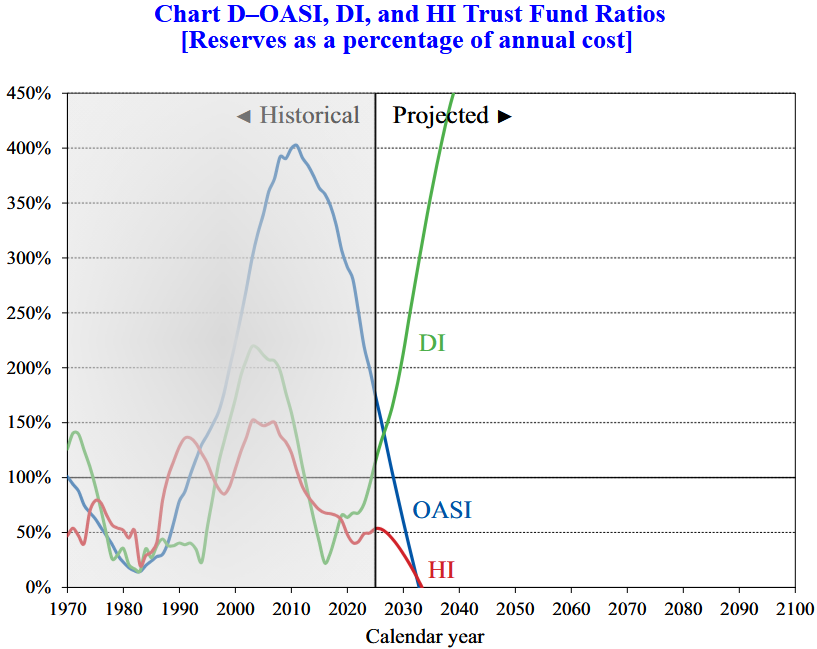
This is where the Trust Funds come in. Before 2010 this was happening, and the excess was earmarked into Trust Funds and invested in Treasuries (non-marketable securities – so only a bookkeeping entry). Since 2010 when payroll tax revenue fell short of outgoing benefits, the difference was made up by drawing down the Trust Funds. Technically the Trust Funds are simply IOU’s from the government but that is a separate, complex topic. It is the year these Trust Funds are projected to go to $0 and the % of promised benefits covered thereafter that summarizes the health of the programs (refer to intro).
Q5 - So how soon will the Trust Funds hit $0? Then what happens?
Very soon! The Old-Age and Survivors Insurance (OASI) Trust Fund is projected to hit $0 in Q4 2032 at which time only payroll tax will be available to pay 78% of promised benefits. If combined with the Disability Insurance (OASDI) Trust Fund (would require Congress to act), funds will be depleted in 2034 and then cover 83% of promised benefits. Medicare Hospital Insurance Trust Fund (Part A) is projected to run out in Q2 2033 and payroll tax is projected to cover 89% of promised benefits. Where is the Trust Fund for Medicare Supplementary Medical Insurance (Part B and D) you ask? It is never projected to be depleted since financing the SMI is set to meet expected costs, again roughly 22% from increasing Medicare premiums, 75% from taxpayer generosity and remaining 3% from various sources (see table in next section).
Q6 - Wait a minute. Tell me about Medicare funding again?
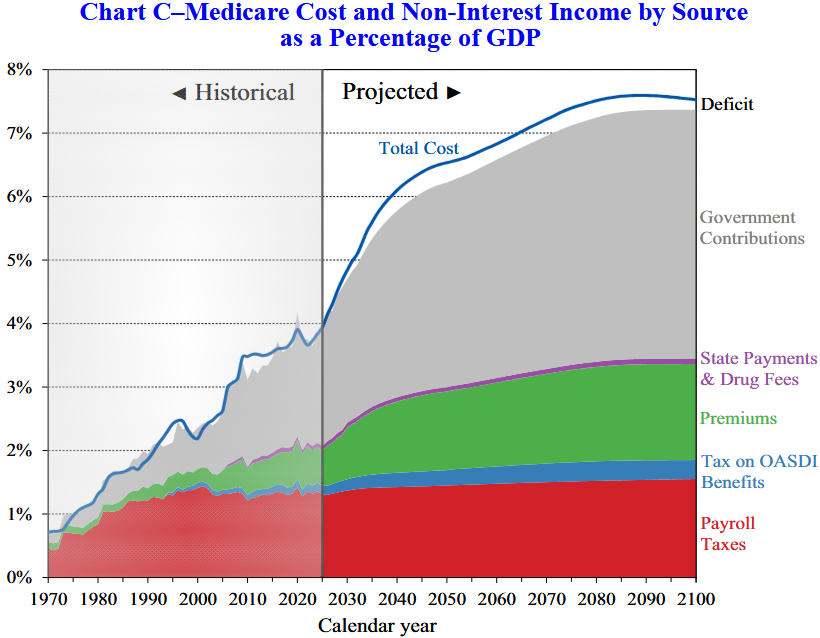
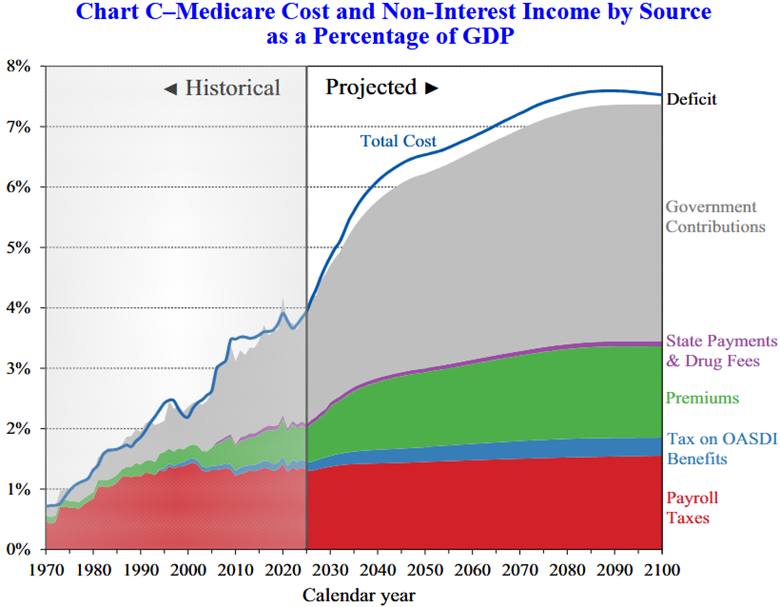
Only the Hospital Insurance (Part A) is funded by payroll taxes (see red area in graph below). The Supplementary Medical Insurance (Part B and D) has about 22% funding from Medicare premiums (green area) and most of the other 78% from general taxing revenue (grey area) and taxes on Social Security benefits (blue area). That is why Medicare Part B premiums seem so reasonable – it only reflects about 22% of the true cost. What is staggering is the projected cost as a % of GDP for the overall program – going from 2% in mid-90’s to about 4% today and surpassing 6% in less than 20 years! Last year’s long-term projections remained below 7% while this year that level is breached in about 2070.
The majority of that long-term expanded cost is projected to be covered by general tax revenue based on current law – not payroll taxes or dedicated premiums. In fact, the law requires Trustees to trigger a “Medicare funding warning” if general revenue is projected to exceed more than 45% of total projected costs in any of the next seven years for two years running. This has happened for NINE consecutive years. The President must submit proposed legislation to Congress to respond to the warning “on an expedited basis”. I mentioned nine consecutive years, right? We already have a large debt problem in our country, partially from the growing gray area to the left of the line below. Notice how much bigger the gray area becomes to the right – and these are % of GDP values.
Q7 - Interesting. Can you briefly explain each of those color bands again?
Note the chart covers both Medicare programs – Hospital Insurance (Part A) and Supplemental Medical Insurance (Part B and D). The bills are paid as follows:
Payroll Taxes (red) – 1.45% FICA tax paid by current workers; plus 1.45% from employer
Premiums (green) – monthly Part B and D premiums once on Medicare; includes IRMAA (see later)
Government Contribution (gray) – money from us, the taxpayers, via general tax revenue; growing!
Tax on OASDI Benefits (blue) – ranges from 0% - 85% of SS benefits are taxable income based on ‘base income’ definition which is too convoluted to summarize here. Note the levels were set in 1983 and NOT adjusted for inflation, so it continues to catch more people at 85% of SS benefits to taxable income:
- Individual filer – 0% if < $25k; up to 50% between $25k - $34k; up to 85% > $34k
- Joint filers – 0% if < $32k; up to 50% between $32k - $44k; up to 85% > $44k
- Interestingly, tax revenue up to 50% of benefits goes to OASDI; rest goes to HI
State payments & Drug Fees (purple) – state contributions if an individual would have been on Medicaid if not for Medicare; not sure of drug fees.
Q8 - You mentioned extra tiered premiums for Medicare Part B and D and IRMAA. What is this?
The 2026 premium for Medicare Part B is $202.90/month and Part D varies by plan based on drug coverage chosen. Due to Medicare financing concerns at the beginning of this century, the Medicare Modernization Act of 2003 introduced Income Related Monthly Adjustment Amounts (IRMAA) for Part B only and first implemented in 2007. It was expanded to Part D in 2010 to help fund Affordable Care Act. The bands and premium adjustments are set by Congress and have been changed over the years. IRMAA applies if Modified Adjusted Gross Income (based on tax return two years ago) is currently above $109k for single and $218k for joint filers. There are multiple tiers, reaching double the premium in the middle tier and 3.4x premium level at the highest tier. I expect Congress will continue utilizing this mechanism to quietly increase financing for Medicare. NOTE: Part B IRMAA shows the total premium; Part D IRMAA shows additional amount above your plan premium since varies for each person based on drug exclusions selected.
Q9 - So should I assume I will get nothing from Social Security?
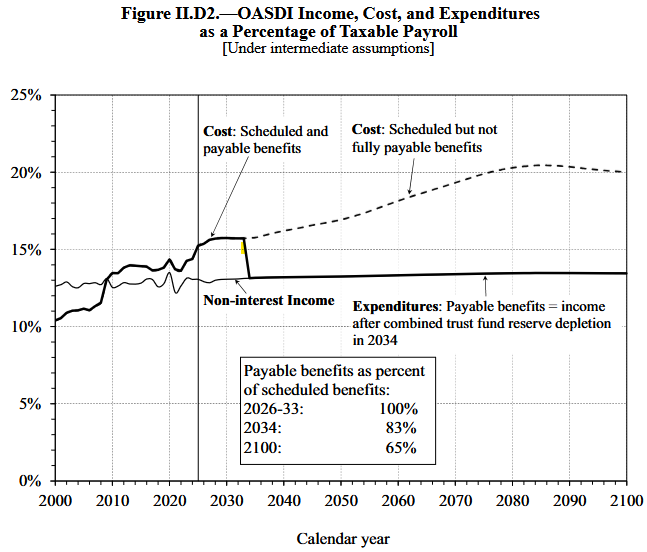
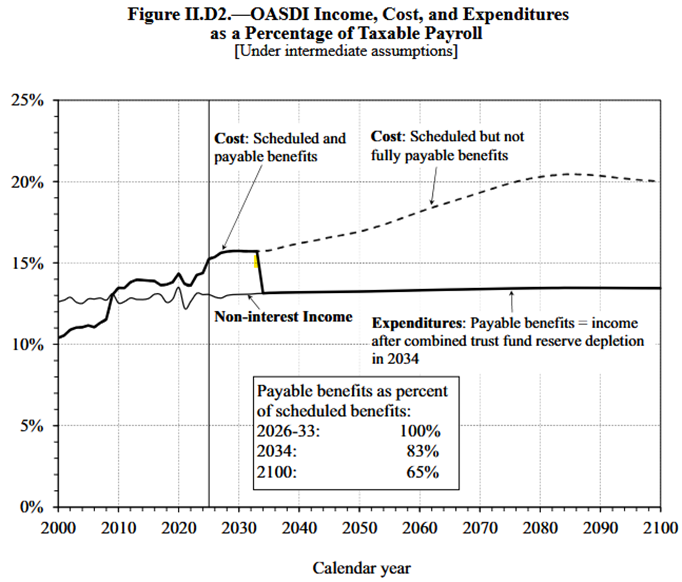
No. I believe for those currently receiving benefits there will be no reduction. For younger workers, you will very likely get less than currently promised but it will be much closer to the promised benefit than it will be to $0. Remember Social Security is a pay-as-you-go system. After the Trust Funds are depleted there is still current payroll tax coming in to pay benefits. The graphic below shows that while there won’t be enough funds to pay the current promises, it will be enough to pay 83% starting in 2034 (using combined OASDI), then drifting down to 65% in 2100 and beyond. In reality it will likely be some combination of lower benefits and higher taxes to avoid this cliff, though given the history, likely tilt toward more taxes since politicians don’t like to cut benefits.
Q10 - I’m in good health and my advisor keeps telling me to delay Social Security. My parents claimed SS at 65 so why shouldn’t I?
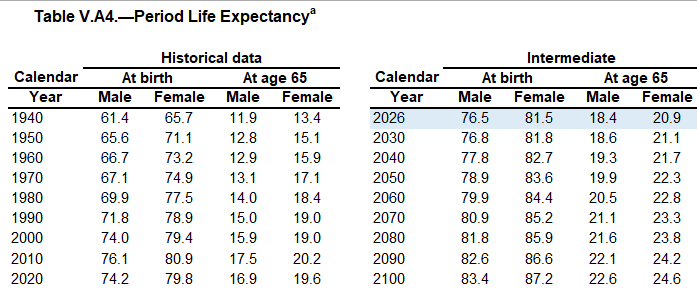
Because you are living longer and your benefit will be reduced by 13% for life if you claim at age 65 instead of full retirement age (FRA) of 67 if born in 1960 or later (FRA was 65 when program first started). Think of Social Security as an inflation-adjusted income payable for as long as you or spouse are alive from a high-quality institution. For those born after 1960, delaying your benefit by just three years will increase this wonderful pension by 24%. Did I mention it also grows with inflation and is payable for life? Get some of that.
The table below shows life expectancy over time. The first two columns show life expectancy at birth; the last two show the expected remaining life expectancy for those who made it to age 65. Notice the increasing life expectancy, both historically and projections.
Q11 - Can’t they just raise payroll taxes to cover the shortfall?
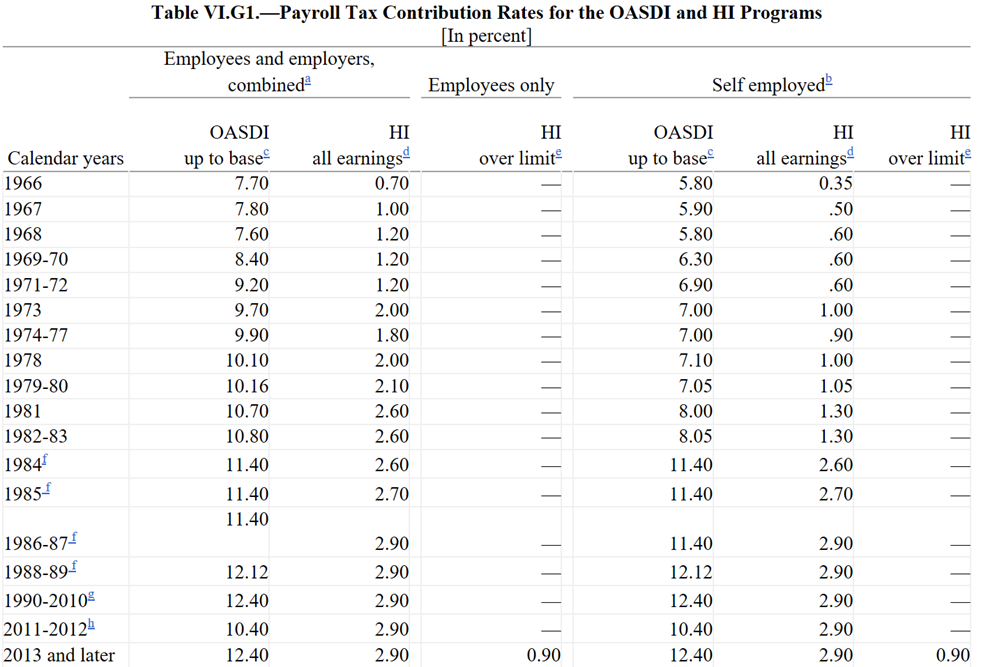
Sure – but the combined rate is already quite high, and much higher than expected when the program began. One projection (using the 2025 Report - see details later) to cover the Social Security shortfall is to increase OASDI payroll tax from 12.4% (6.2% x 2) to 16.4% (extra 4.0% of your income) starting now. Adding the 2.9% Medicare + extra 0.90% for high earner moves the total FICA tax to 20.2% - over one-fifth of payroll! – to fund the ever-increasing benefits. The table below shows the historic OASDI and HI payroll tax rates since the mid-60’s. It is important to recall the original intent of Social Security was to keep individuals out of poverty, not to provide full retirement income for most Americans. It is difficult to make changes when the impact is so far down the road, but the day of reckoning is upon us. A healthy debate is needed about what % of total income should be forced into a government program that provides a necessary safety net to keep people out of poverty and leave the remaining amount in the hands of the individual.
Q12 - Can’t they just raise taxes on the high income earners?
It is important to realize both Social Security and Medicare are already doing this in a few ways. Before adding even more progressive features, it is important to understand and acknowledge the built-in progressive elements of the program.
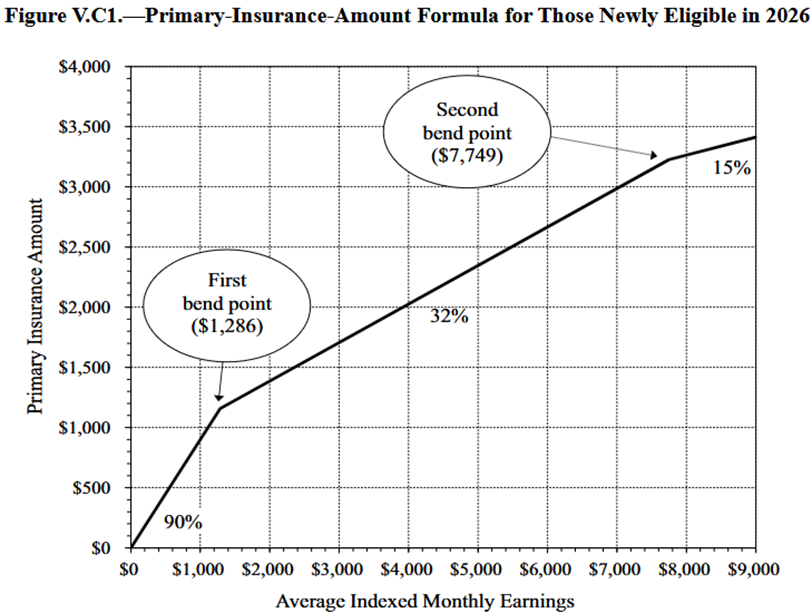
- Social Security uses “bend points” to calculate the benefit received. Everyone pays the same 6.2% FICA tax on income (up to caps) but the benefit is based on a % of earnings, with a higher % payout for lower earnings. Specifically, 90% of the first $1,286 in monthly earnings is paid as a benefit, then 32% on income between $1,286 - $7,749, and finally 15% above. This results in lower income workers receiving a much higher % of their income as a benefit even though all paid the same %. Keeping with the “social” part of the program and lifting individuals out of poverty makes sense. But it should be recognized that the benefit calculation is already quite progressive and raising the salary cap for FICA only provides 15% of those earnings as benefit, vs. the 90% at lower levels (see graph below).
- A portion of Social Security benefits is included in taxable income if ‘base income’ exceeds thresholds. See the earlier discussion. Recall these thresholds ARE NOT adjusted for inflation so it will continue to catch more people having to apply 85% of SS benefits to taxable income. Note $35,700 was the maximum wage limit for Social Security taxes in 1983 when these thresholds were set. That wage limit today adjusted for inflation is $184,500, so you can see the expanded pool of individuals now exposed to taxable SS benefits relative to when first passed. Also recall the recent extra 0.90% Medicare tax on earnings above $200k single and $250k joint is NOT indexed to inflation either.
- Medicare collects a higher monthly premium on high income beneficiaries by something called IRMAA. See the earlier discussion. Here is a link to the cost section of the Medicare website.
Q13 - What changes to Social Security are being considered and what is the impact on funding?
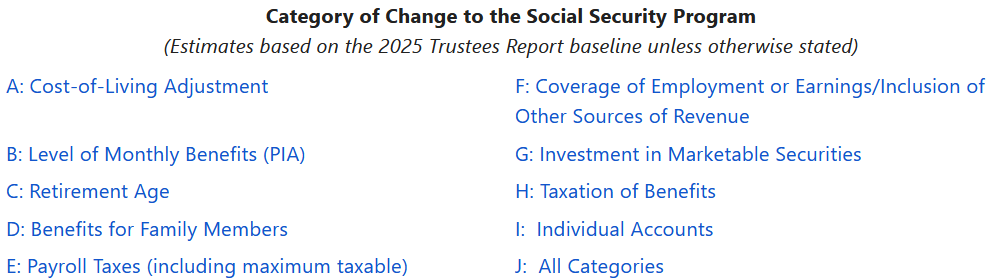
There are different changes being considered to the Social Security program. A summary of the changes and the financial impact to the program is summarized by the Office of the Chief Actuary and can be found here (estimates based on 2025 Trustees Report).
Below is a list of the nine different areas where reforms could be focused. It will likely require some combination of these changes in order to assure long-term financial stability. Note these are only Social Security changes, not Medicare. Also notice they list “Individual Accounts” as a category. While not stated, it will be interesting to see if this program looks toward the new Trump Accounts being funded for young children as an example of how it could be incorporated.
If you are still with me I hope this was helpful. It is important to be aware of the issue to not only help plan your retirement (don’t assume $0 Social Security benefit!) but also to engage in a thoughtful, well-informed debate about the best path forward for these important, yet financially troubled programs. I don’t believe they will change the benefits for those already or close to receiving benefits as I am reminded of a then Senator Rubio comment during a presidential debate years ago – “I’m against anything that’s bad for my mother.”
Have questions? Reach out! We're happy to help.
Posted by Kirk, a fee-only financial advisor who looks at your complete financial picture through the lens of a multi-disciplined, credentialed professional. www.pvwealthmgt.com